
OVERVIEW
Payer connectivity and orchestration for the full claim lifecycle
For revenue cycle teams, working with payers rarely follows a single channel or workflow. We act as a connectivity and orchestration layer, routing work across APIs, EDI, clearinghouses, portals, and specialist-assisted handling. Then we normalize outcomes and return them to your systems, keeping everything aligned and actionable.
Instead of relying on one method or targeting just one part of the process, we combine multi-channel connectivity, intelligent routing, fallback options, and outcome normalization. The result? Consistent answers and fewer surprises from start to finish.
Our approach supports the full claim lifecycle, so work keeps moving without your team bouncing between portals, calls, faxes, emails, and spreadsheets. What’s included:
Pre-service: Eligibility, benefits, prior authorization
Mid-cycle: claim submission support, claim status, rejections triage
Post-service: denials, appeals, remittance, payment posting, A/R follow-up
It all adds up to a consistent way to connect with payers, reduce manual work, and improve visibility from the first check to the final payment.

THE PROBLEM
Why manual payer follow up breaks at provider organizations scale
Most providers still rely on a mix of portals, phone calls, and fax based exchanges to move payer work forward. That approach is hard to scale and hard to govern because outcomes are inconsistent and tracking lives outside core systems.
What manual payer work creates:
- Unreliable status visibility, the same account gets worked by multiple teams because there is no shared source of truth
- Delays from call queues, call backs, limited payer hours, and payer specific steps
- Documentation gaps, missing faxes, incomplete packets, and lost confirmations that drive rework and denials
- Missed deadlines for follow up, resubmissions, and appeal windows because tracking is manual
- Limited auditability because evidence is scattered across notes, inboxes, and files
We replace ad hoc payer chasing with routed execution, exception handling, and structured outcomes back into your systems.
Coverage
Connected across payers and delegated administrators
Many payers delegate key parts of the revenue cycle experience to third parties, especially for authorization, medical necessity, and guideline-driven workflows. That is why we support 2800+ payer connections alongside clearinghouses and utilization management partners, including benefit managers and third-party administrators.
This helps your teams follow the path the payer requires, even when it is routed through a delegated administrator. Examples include, varies by plan, workflow, and client configuration.

EviCore
Availity
AIM, Carelon
Optum
NIAMagellan
HealthHelp
APPROACH
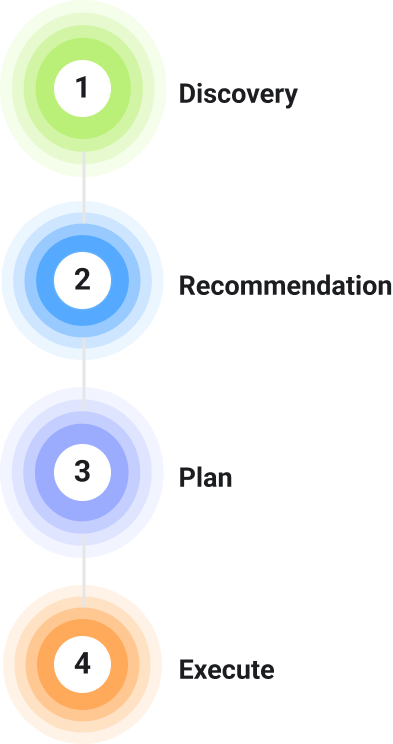
A consultative path from discovery to execution
Payer connectivity works best when it is designed around your payer mix, workflows, and system constraints. Infinx starts with discovery, then recommends the right paths, then plans and executes in phases.
How we engage:
- Discovery – align on workflows in scope, payer mix priorities, delegated administrator paths, and what done means
- Recommendation – map each payer and workflow to the most reliable channel, define fallbacks, and confirm the data we will return
- Plan – define integration patterns, security and access requirements, validation steps, and rollout sequencing
- Execute – implement routing, automation, exception handling, and write back, then expand lane by lane
This keeps implementation practical, measurable, and aligned to how work is actually performed.
HOW WE CONNECT
Multi channel connectivity, built for real payer behavior
No single method covers every payer and workflow. We use a multi-channel approach, so you get reliable coverage across your payer mix and do not lose throughput when a payer does not support the ideal path. You get practical coverage that matches how payer work actually happens, not just how it is supposed to happen.
Connectivity methods we support:
API connections where available for the payer and workflow
Clearinghouse connectivity for broad access and standardized exchange
EDI transactions where supported for the workflow, for example eligibility 270 and 271, claim status 276 and 277, authorization 278, claims and remits 837 and 835
Payer and utilization management portals executed through automation and guided workflows
Secure file-based exchanges such as batch and SFTP
Specialist assisted handling when a payer requires calls, attachments, documentation nuance, or manual steps
ORCHESTRATION
Routing, fallbacks, and outcomes that keep work moving
Connecting is only step one. The bigger challenge is ensuring every request follows the right path, responses are interpreted consistently, and exceptions do not stall the queue.

How payer work is orchestrated:
- Payer and workflow mapping to select the right channel and required fields
- AI-assisted payer mapping and normalization to keep routing accurate across payer aliases and delegated administrator paths
- Channel selection that is specific to the payer and workflow, with fallbacks when the primary path fails or returns incomplete data
- Automated execution for repeatable tasks such as lookups, submissions, and status checks
- Controlled retries and monitoring to surface portal failures, authentication issues, and data gaps quickly
- Exception routing to specialists for unclear responses, missing data, or documentation needs
- Standardized outcomes that translate payer replies into consistent statuses and next steps
This turns payer variability into a managed process, so teams spend less time chasing and more time resolving
MANAGED SERVICE
Connectivity that stays healthy over time
In provider environments, payer portals often change, credentials can expire, and workflows vary by plan. These moving parts can lead to disruptions and take time away from your team’s day-to-day responsibilities. We manage payer connectivity as part of Healthcare Revenue Cloud, helping to reduce that burden and keep things running smoothly.
As payer requirements evolve, this approach helps maintain consistent performance and minimizes the need for manual troubleshooting. Here’s what that includes:
Proactive Monitoring
Monitoring and alerting across connectivity channels to catch failures early
Ongoing Maintenance
Ongoing maintenance of routing logic, mappings, and workflow rules as payer requirements change

Credential Handling
Credential and session handling support for portal based workflows, including
Operational Reporting
Reporting to show throughput, failures, and resolution patterns over time
AI-Assisted Mapping
Payer mapping and normalization identifies payer aliases and administrators, routing workflows through the best channel with traceable, human-reviewed exceptions

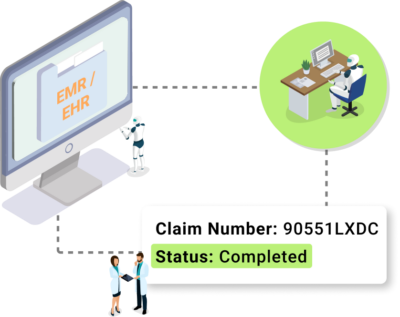
RETURNED DATA
Structured results back into the systems your teams use
Payer responses arrive as portal statuses, free text, attachments, and inconsistent labels. Infinx normalizes those outcomes into structured fields, then delivers updates back into your workflow so downstream teams can act without rework.
Typical updates delivered back to your workflow:
- Standardized status and disposition fields for prioritization
- Key payer and case data captured consistently per workflow requirements
- Notes, timestamps, and documentation references for traceability
- Action history to support audits and internal handoffs
- Optional raw response retention where needed for troubleshooting or compliance workflows
When outcomes are structured, teams can route work faster, measure performance more accurately, and reduce preventable delays.
WHAT WE NEED FROM YOU
A few inputs to make payer connectivity work well in provider environments
To make implementation smooth and outcomes consistent, we align on a short set of operational and technical inputs up front, so we can map the right path by payer and workflow, validate write back, and avoid surprises during rollout.
- Workflows in scope and what done means for each workflow
- Payer mix priorities, plan types where relevant, and delegated administrator paths
- Identifiers and routing details as applicable, for example NPI, TIN, payer IDs, receiver IDs
- Clearinghouse relationships and configuration where applicable
- Portal access and credentials, including how MFA is handled
- Documentation rules and attachment requirements for prior authorization and appeals
This keeps rollout predictable and avoids surprises during validation.
END TO END WORKFLOWS
Payer connectivity that supports the full claim lifecycle
Different teams touch payer systems at different points, but they should not need different tools and processes to get answers. We support payer connectivity across pre service, mid cycle, and post service work, using the same routing and normalization approach.
Where this shows up across revenue cycle work:
- Patient access, eligibility and benefits validation, prior authorization initiation and follow up, status tracking
- Claims and rejections, claim status retrieval, rejection triage, follow up workflows based on payer disposition
- Denials and appeals, portal and documentation workflows, submission tracking, consistent outcome capture for reporting
- Payments and posting, remittance driven workflows, reconciliation support, exception handling for posting readiness
- A/R follow up, scaled status retrieval and categorization, prioritization of accounts that need human judgment
This creates a continuous payer connectivity layer that supports performance from scheduling through final payment.
PROVIDER INTEGRATIONS
Fit your EMR, billing, and analytics ecosystem
You should not have to add another silo to gain payer connectivity. Infinx is designed to integrate with the systems you already run, and to return outcomes in formats that match your operational and IT requirements.
Common integration patterns:
API Integration
API based integrations for workflow updates and data exchange
HL7 and FHR
HL7 and FHIR where applicable for EMR, PMS, and downstream workflow updates
SFTP Exchanges
Secure batch and SFTP exchanges for files, extracts, and bulk updates

Structured Exports
Structured exports for reporting, reconciliation, and downstream automation
IMPLEMENTATION
Start with one lane, then expand with confidence
Payer connectivity programs succeed when they start with discovery and clear workflow outcomes, then expand in phases across a representative payer set. We typically begins with a focused lane, then expands once routing, exception handling, and write back are stable.
A practical way to roll out:
- Align on workflows in scope and what done means for each
- Confirm payer mix priorities, channels, credentials, and documentation rules
- Validate outputs, write back, and exception handling with the teams who rely on the data
- Expand coverage by workflow, payer group, and site after stabilization
This approach reduces risk, speeds time to value, and avoids disruption to daily operations.

SECURITY
Designed for PHI, governance, and auditability
Payer connectivity touches PHI and affects cash, compliance, and patient experience. Infinx supports strong controls and traceability so organizations can deploy confidently across teams, locations, and specialties.
Operational security and governance support includes:
- Role based access aligned to job function
- Audit logs and action traceability across payer touches
- Encryption in transit and at rest
- Monitoring to surface failures and exceptions quickly
This helps IT, compliance, and revenue cycle leaders align on a scalable, accountable model.

Faq
Payer connectivity questions, answered
Payer connectivity gets complicated fast once you factor in delegated administrators, portal variance, and workflow specific requirements. These FAQs cover how we connect, how we keep connectivity healthy over time, and how outcomes flow back into your systems across the full claim lifecycle.
See how we connect to your payer mix
If payer work is slowing down authorizations, claim velocity, denial resolution, posting, or A/R performance, we will start with a short discovery to understand your payer mix, delegated administrators, workflows, and target systems. From there, we will recommend the right connectivity paths by payer and workflow, then propose a rollout plan and execute with validation and expansion by lane.